In the competitive world of PET imaging modality, copper-64 (Cu-64) tracers are emerging as a compromise between the tracers from two commercial isotopes gallium-68 (Ga-68) and fluorine-18 (F-18). Leveraging their logistical flexibility, favorable half-life, and good image quality, Cu-64-based tracers are currently under active clinical investigation for applications in neuroendocrine tumors and prostate cancer imaging.
When selecting a PET radiotracer, clinicians consider balancing physical decay characteristics, image quality, logistical constraints, and patient safety. Ga-68, F-18, and Cu-64 tracers each offer unique strengths and trade-offs, including differences in half-life, cost, image resolution, and radiation dose. Table 1 compares attributes of these tracers.
Table 1: Comparison of Ga-68, F-18 and Cu-64 PET Tracers

Ref 1: National Nuclear Data Center, Brookhaven National Laboratory, https://www.nndc.bnl.gov/
Ref. 2: From Package Insert, Illuccix and Pylarify: https://illuccixhcp.com/wp-content/uploads/illuccix-prescribing-information.pdf, https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/214793s000lbl.pdf
Ref. 3: From a clinical study public information: https://www.clinicaltrials.gov/study/NCT05653856?tab=table#trial-description
Ref. 4: Calculated assuming activity of 5 half-lives at the time of manufacture at the upper limit of dosage
Ref. 5: Based on positron range of 2.9 mm, 1.0 mm and 0.6 mm for Ga-68, F-18, and Cu-64 tracers respectively
A pictorial representation of select key parameters is shown in Figure 1 below.
Figure 1: Half-life, Usage Window and Positron Yield of Ga-68, F-18, and Cu-64 tracers
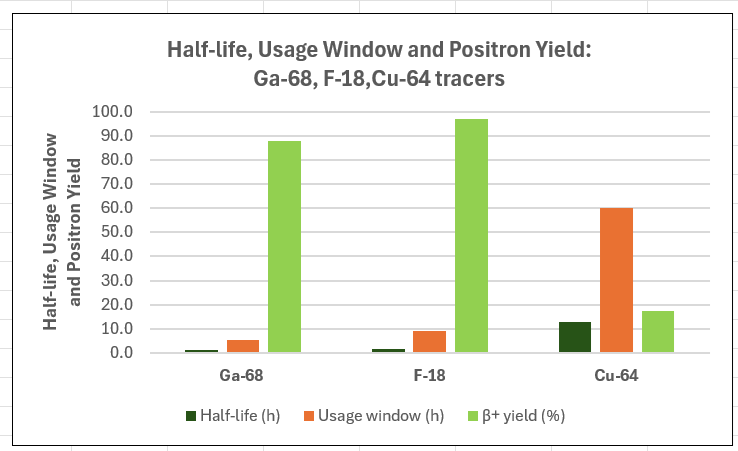
Ga-68 tracers are relatively low-cost, require on-site/close to site production and have a relatively tight window for patient scheduling. F-18 tracers provide high-quality imaging, a moderate yet sufficient distribution range, and a longer usable time window, making them well-suited for clinical workflows. Cu-64 tracers strike a balance—providing superior logistical flexibility, good resolution, and lower cost.
Despite its promise, Cu-64 tracers present unique challenges including mixed decay pathways, with β electron radiation exposure that warrant careful consideration. The following discussion outlines key advantages and limitations of Cu-64 tracers for clinical PET imaging.
Pros & Cons of Cu-64 Tracers
Pros:
- High tumor-to-background ratios: Clinical studies of Cu-64-SARTATE vs. Ga-68-DOTATATE in GEPNETs demonstrated superior signal to noise ratio in phase II “DISCO” clinical trial, which translates to superior sensitivity for the detection of smaller lesions (ref.).
- Theranostic potential: Copper has both imaging (Cu-64) and therapeutic (⁶⁷Cu) isotope, allowing identical matched theranostic pairing that have closely matched pharmacokinetic and pharmacodynamic behaviors.
- Uptake time: Higher flexibility to allow longer uptake time of 2-3 hours if warranted
Cons:
- Lower positron yield (~17.5%): Cu-64 has fewer positron emissions per decay activity and may require longer scan times for equivalent dosage
- Specificity: May be lower due to higher sensitivity
- Beta and Auger emissions: Patient exposure may be a concern; these are negligible for F-18 and Ga-68 tracers.
- Physiological clearance time: This may be higher compared to Ga-68 and F-18 tracers due to longer half-life.
Conclusion
Cu-64 tracers offer a middle ground between the short-lived, rapid-turnaround Ga-68 and the high-resolution, intermediate half-life but costlier F-18 tracers. With a longer half-life, lower cost, enhanced sensitivity, and theranostic pairing potential, Cu-64 tracers are well-suited for remote-site imaging while offering greater scheduling flexibility.
However, these benefits come with additional patient exposure from beta and Auger electron emissions, which warrant further clinical evaluation.
In practical settings, the adoption of Cu-64 PET tracers should be guided by factors such as supply chain considerations, operational convenience, scanner availability, patient throughput, radiation safety considerations, and the required imaging performance for specific clinical indications.